ЦЕЛИ:
Сравнить результаты УЗИ энтезов у пациентов с анкилозирующим спондилитом (АС) со здоровыми контрольными лицами и оценить способность ультразвука (УЗ) идентифицировать аспекты, связанные с заболеванием.
МЕТОДЫ:
Было проведено перекрестное исследование с участием 50 пациентов с АС и 30 здоровых пациентов. Клиническая оценка включала в себя использование визуальной аналоговой шкалы боли, оценку отека энтезов, подробное интервью для пациентов и врачей, использование индекса активности заболевания, показателей подвижности и дисфункции, скорости оседания эритроцитов и клинического индекса энтезита.
УЗИ проводилось двумя опытными скелетно-мышечными радиологами для следующих энтезов: плечевых трицепсов, дистальных четырехглавых, проксимальных и дистальных сухожилий надколенника, пяточных сухожилия и фасции; для оценки использовались сумма и подпункты Мадридского сонографического индекса энтезита.
РЕЗУЛЬТАТЫ:
Сравнение между группами показало статистически значимое различие с худшими показателями у пациентов с АС, с эрозией кости пяточного энтеза и эрозией кости и утолщением подошвенной фасции. Перевес разницы утолщения подошвенной фасции в группе АС составил 3,47 согласно логистическому регрессионному анализу. Группа АС также имела худшие оценки в отношении наличия кальцификации в четырехглавой мышце с пятикратно повышенным риском.
ЗАКЛЮЧЕНИЕ:
Сонографический анализ, показал, что только по энтезам стопы и четырехглавой мышцы возможно отдифферинцировать пациентов с АС от здоровых людей.
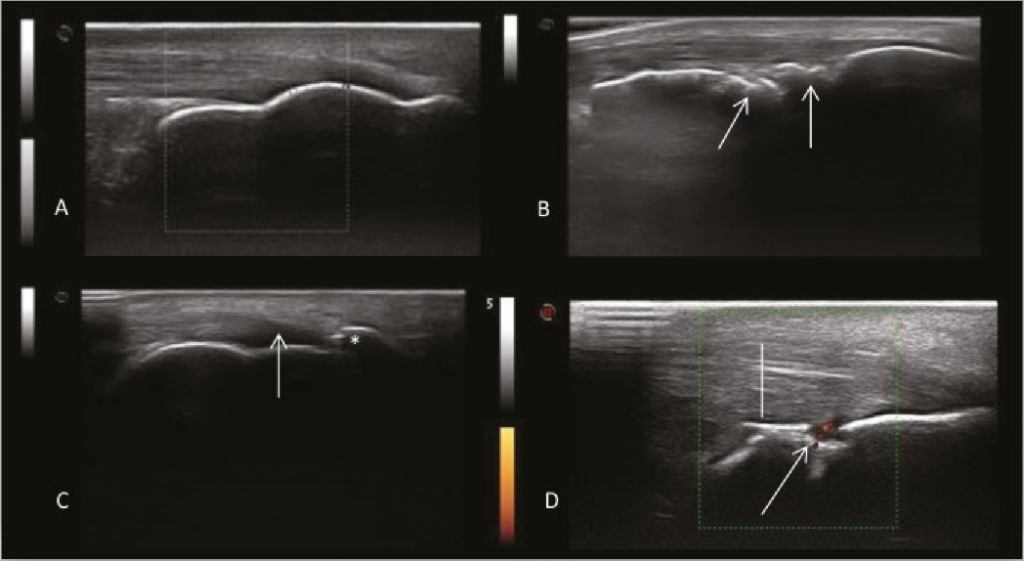
А. Нормальный вид пяточного энтеза. B. Костные нарушения и кальцификация. C. Образование энтезофитов (*) и потеря фибриллярного рисунка пяточного сухожилия (↑). D. Эрозия кости с сигналом PD (↑) и утолщением сухожилия (|). Рисунок 1. Ультразвуковые изображения пяточного энтеза.
Suellen Narimatsu Ishida, Rita Nely Vilar Furtado, André Rosenfeld, Jorge Ernesto Passos Proglhof, Germana Brigida Queiroga Estrela, Jamil Natour
Clinics (Sao Paulo). 4 Apr 2019; vol. 74: e727
DOI: 10.6061/clinics/2019/e727
![]()
Ultrasound of entheses in ankylosing spondylitis patients: The importance of the calcaneal and quadriceps entheses for differentiating patients from healthy individuals
OBJECTIVES:
To compare the ultrasonographic findings of entheses in ankylosing spondylitis (AS) patients with those of healthy control individuals and to assess the ability of ultrasound (US) to identify aspects related to the disease.
METHODS:
A cross-sectional study involving 50 patients with AS and 30 healthy controls was performed. Clinical assessment included the use of a visual analog scale for pain, assessment of swelling of the enthesis, global assessments for patients and physician, use of a disease activity index, mobility and dysfunctional indices, erythrocyte sedimentation rate and clinical enthesitis index.
US was performed for the following entheses by two experienced musculoskeletal radiologists: brachial triceps, distal quadriceps, proximal and distal patellar tendons, calcaneal tendon, and plantar fascia; the total and subitems of the Madrid Sonographic Enthesitis Index were used for evaluations.
RESULTS:
Comparison between groups showed a statistically significant difference with worse scores in AS patients, with bone erosion of the calcaneal enthesis and bone erosion and thickening of the plantar fascia. The odds ratio for thickening of the plantar fascia in the AS group was 3.47, according to logistic regression analysis. The AS group also had worse scores regarding the presence of calcification in the quadriceps enthesis, with a fivefold increased risk.
CONCLUSION:
US analysis showed that only entheses of the foot and quadriceps were able to differentiate AS patients from healthy individuals.
A: Normal aspect of the calcaneal enthesis. B: Bone irregularities and calcification. C: Enthesophyte formation (*) and loss of the fibrillar pattern of the calcaneal tendon (arrow). D: Bone erosion with PD signal (arrow) and thickening of the tendon (bar). Figure 1: Ultrasound images of the calcaneal enthesis.